BIMONTHLY ASSIGNMENT MAY 2021
|
Jan, 20
yrs ago |
·
Her first SOB
episode ·
Lasted one week ·
Relieved on
taking medication
|
|
Jan, 19
years ago Jan, 18
yrs ago Jan 17
yrs ago Jan, 16
yrs ago Jan, 15
yrs ago Jan, 14
yrs ago Jan, 13
yrs ago
|
·
Similar
episodes ·
SOB lasted approximately
one week ·
All episodes
were relieved upon taking medication
|
|
Jan, 12
yrs ago
|
·
Lasted 20 days ·
Episode of SOB ·
Hospitalised ·
SOB decreased
upon treatment in the hospital
|
|
Jan, 11
yrs ago Jan, 10
yrs ago Jan, 9
yrs ago
|
·
SOB episodes ·
Lasting almost
a month
|
|
8 yrs ago
|
·
Polyuria (
diagnosed as DM) ·
Diagnosed with
diabetes |
|
Jan, 7
yrs ago Jan, 6
yrs ago Jan,5
yrs ago
|
·
SOB episodes ·
Lasting almost
a month
|
|
5 yrs
ago
|
Treated
for anemia with iron injections |
|
Jan, 4
yrs ago Jan, 3
yrs ago Jan, 2
yrs ago Jan , 1
yr ago
|
·
SOB episodes ·
Lasting almost
a month
|
|
30 days
ago |
·
Latest episode
of SOB ·
SOB was
insidious in onset and gradual in progression Initially
SOB occurred on exertion and was relieved upon rest ·
Generalised weakness(
administered IV fluids by a local rmp) |
|
20 days
ago |
·
Patient got HRCT
done outside which showed signs of bronchiectasis ·
Diagnosed with
hypertension |
|
15 days
ago |
·
Pedal edema
upto ankle, pitting type ·
Facial puffiness |
|
2 days
ago |
·
SOB at rest
(grade 4) and was not relived with nebulisers ·
SOB progressed (the
patient’s SOB is usually relieved with the use of nebulisersand inhalers but
that did not happen in this episode) ·
Drowsiness ·
Decreased urine
output
|
anatomical location - lungs and the airways
etiology: the primary etiology of the patient's problem could be the the occupation of the patient . The patient works in a paddy field which increases the risk of being exposed to fine dust. Prolonged exposure to the dust can cause COPD (most common cause being smoking)
QUESTION: What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
ANS) 1)Head end elevation_ 30-45°
. It is recommended in this patient since she is on mechanical
ventilation to reduce the incidence of VENTILATOR ASSOCIATED PNEUMONIA that
occurs due to aspiration of contaminated oropharyngeal secretions following
endotracheal tube intubation.
Efficacy based on studies: Moderate quality evidence from eight studies involving 759 participants demonstrated that a semi-recumbent (30º to 60º) position reduced clinically suspected VAP by 25.7% when compared to a 0° to 10° supine position.
2)O2 inhalation-
It is given for this patient as her spo2 levels at the time of presentation were 75% at room air
.Indication for o2 inhalation: supplemental o2 therapy / inhalation is
given when spo2 levels are below <92% at room air.
3)Intermittent BiPAP-
Bilevel positive airway pressure (BiPAP) ventilation is a non invasive technique used to provide support to a spontaneously, but insufficiently, breathing patient using a nasal mask.
MOA:
BiPap machine supplies pressurized air into your
airways. It is called “positive pressure ventilation” because the device
helps
open your lungs with this air.
The machine has 2 pressure settings
1) for inhalation IPAP
2) low pressure foe exhalation EPAP
.Indication: it is given to the patient to provide respiratory support
as she is diagnosed with COPD.
4)Injection Augmentin 1.2gm IV /BO
.It is given to the patient to treat Broncheictasis
.augmentin is a combination of
AMOXICILLIN- binds to penicillin binding proteins in
bacterial cell wall and thereby inhibits bacterial cell wall
synthesis.
CLAVULINIC ACID - is a beta lactamase enzyme
inhibitor , thereby facilitates action of Amoxicillin.
MOA-
Amoxicillin binds to penicillin-binding
proteins within the bacterial cell wall and inhibits bacterial cell wall
synthesis. Clavulanic acid is a β-lactam, structurally related to penicillin,
that may inactivate certain β-lactamase enzymes.
5)Tab. Azithromycin 500mg OD
.It is given to the patient to provide symptomatic relief and reduce incidence of acute exacerbations of COPD.
MOA-
Azithromycin binds to the 23S rRNA of the bacterial 50S ribosomal
subunit. It stops bacterial protein synthesis by inhibiting the transpeptidation/translocation
step of protein synthesis and by inhibiting the assembly of the 50S ribosomal
subunit
EFFICACY BASED ON A STUDY:
A randomized controlled trial found
that patients hospitalized for an acute exacerbation of chronic
obstructive pulmonary disease (COPD) experienced reduced rates of treatment
failure when adding azithromycin to their standard of care.
During the study, patients received a low dose of azithromycin in addition to their prescribed medications while in the hospital and continued taking the antibiotic for 3 months following hospitalization. The result, according to the data, was reduced treatment failure compared with standard of care alone. Rates of treatment failure were under 50% for patients taking azithromycin (49%) compared with 60% for patients receiving standard of care.
6)INJ. LASIX IV BO if SBP greater than 110 mmHg
.It is given to the patient to relieve symptoms of fluid
retention(edema)
.It is also used to treat hypertension
.MOA:
Furosemide(LASIK) acts by inhibiting the luminal
Na-K-Cl cotransporter in the thick ascending limb of the loop
of Henle,
⬇️
increase the
excretion of Na+ and water by the kidneys
⬇️
Increased urine output
7)TAB PANTOP 40mg PO OD
MOA-
The mechanism of action of pantoprazole is to inhibit the final step in gastric acid
production. In the gastric parietal cell of the stomach, pantoprazole covalently binds to the H+/K+ ATP pump to
inhibit gastric acid and basal acid secretion. The covalent binding prevents
acid secretion for up to 24 hours and longer.
8)INJ. HYDROCORTISONE 100 mg IV
. It acts by reducing inflammation in the body
MOA-
Hydrocortisone binds to the glucocorticoid receptor leading to
downstream effects such as inhibition of phospholipase A2, NF-kappa B, other
inflammatory transcription factors, and the promotion of anti-inflammatory
genes.
Based on a study in comparison to placebo,
systemic corticosteroids
1)improved airflow,
2) decreased the rate of treatment failure and risk of
relapse
improved symptoms and decreased the length of hospital stay.
EFFICACY:
In this study, patients hospitalized with acute respiratory
insufficiency and COPD were randomized to receive either intravenous
(IV) corticosteroid (n=22) or matching placebo (n=22) for 72 hours. All
patients received standardized treatment consisting of
oxygen, aminophylline, nebulized isoproterenol, and antibiotics.
The mean percentage change in both pre- and postbronchodilator forced
expiratory volume in 1 second (FEV1) was significantly greater in patients
receiving corticosteroid in comparison to placebo at all measured time
points.
9)NEB. with IPRAVENT, BUDECORT 6 hrly
MOA-
ipravent belongs to
a group of medicines known as anticholinergic bronchodilators, work by relaxing the bronchial tubes that
carry air in and out of your lungs and makes breathing less difficult.
BUDECORT (Budesonide ) belongs to a group of
medicines called 'corticosteroids'. It works by reducing and preventing
swelling and inflammation in your lungs’.
EFFICACY-
Efficacy based on a study where Patients received 2 mg
of budesonide every 6 h (n = 71),placebo (n = 66). All received
standard treatment,
including nebulized beta(2)-agonists, ipratropium bromide,
oral antibiotics, and supplemental oxygen. The mean change (95% confidence
interval) in postbronchodilator FEV(1) was greater with active
treatments than with placebo: budesonide versus placebo, 0.10 L (0.02
to 0.18 L)
10)TAB PULMOCLEAR 100 mg PO OD
Pulmoclear Tablet is a
combination of two mucolyticmedicines:
1) Acebrophylline
2) Acetylcysteine.
It thins and loosens mucus (phlegm) making it easier to cough
It also relaxes the airway muscles and thereby promotes easy inflow and
outflow of air
11)chest physiotherapy
Chest physiotherapy improves lung
function . ChestPT, or CPT
expands the lungs, strengthens breathing muscles, loosens and improves drainage
of thick lung secretions.
12)GRBS 6 hrly -
.to monitor blood sugar levels
13)INJ. HAI SC ( 8 am- 2pm- 8pm)
Human Actrapid Injection
contains human insulin(short acting)
It is given to the patient to lower blood sugar levels as she is a
diabetic.
14)Temp, BP, PR, SPO2 monitoring
15)I/O charting -
Is used to record fluid
intake and output
16)INJ. THIAMINE 1 amp in 100 ml of NS
MOA-
Thiamine combines with adenosine triphosphate (ATP) in the
liver, kidneys, and leukocytes to produce thiamine diphosphate. Thiamine diphosphate acts as a coenzyme in carbohydrate
metabolism, in transketolation reactions, and in the utilization of hexose in
the hexose-monophosphate shunt.
EFFICACY-
Based on a study- The administration of a single
dose of thiamine was associated with a trend toward increase in oxygen
consumption in critically ill patients
.thiamine deficieny is seen in patients taking loop
diuretics(lasik), as this patient is receiving LASIK, the use of thiamine could
be prophylactic.
The patient has three factors causing an exacerbation:
2. 2)The patient is a known case of hypertension this
can lead to an increase in the pressure of the pulmonary artery. The resulting
hypoxia will further exacerbate the condition leading to right sided heart
failure
3. 3)She also is a known case of diabetes which is a
risk factor
What could be the causes for her electrolyte imbalance?
Answer:
The cause of Hyponatraemia and Hypochloremia can be due vigorous high ceiling diuretic therapy in order to control right heart failure.
QUESTION: What is the evolution of the
symptomatology in this patient in terms of an event timeline and where is the
anatomical localization for the problem and what is the primary etiology of the
patient's problem?
The evolution
of the symptomatology is as follows:
|
1 year ago |
First episode
of seizure
|
|
4 months ago |
Second
episode of seizure (24 hours after with the withdrawal of alcohol, leading to
restlessness, sweating and tremors)
|
|
9 days ago |
Started
talking and laughing to himself, decreased food intake, unable to recognize
family members, has short term memory loss.
|
Anatomical
localization: There are lesions in the peripheral and central nervous system
Etiology:
Since
the Patient has a history of consumption of alcohol, this will lead to a
deficiency in thiamine. A thiamine deficiency gives rise to Wernicke’s
Encephalopathy.
https://www.ncbi.nlm.nih.gov/books/NBK470344/
https://med.virginia.edu/ginutrition/wp-content/uploads/sites/199/2014/06/ThomsonArticle-09.pdf
Thiamine,
also known as Vitamin B1, is a coenzyme that is essential for intricate
organic pathways and plays a central role in cerebral metabolism. This vitamin
acts as a cofactor for several enzymes in the Krebs cycle and the pentose
phosphate pathway, including alpha-keto-glutamic acid oxidation and pyruvate
decarboxylation. Thiamine-dependent enzymes function as a connection between
glycolytic and citric acid cycles. Therefore, deficiency of thiamine will lead
to decreased levels of alpha-keto-glutarate, acetate, citrate, acetylcholine
and accumulation of lactate and pyruvate. This deficiency can cause metabolic
imbalances leading to neurologic complications including neuronal cell death.
QUESTION: What are mechanism of action,
indication and efficacy over placebo of each of the pharmacological and non-pharmacological
interventions used for this patient?
1)IVF
NS and RL @150ml/hr
- Normal saline and ringer lactate solutions are both crystalloid fluids. NS contains 154 mM Na+ and Cl-, with an average pH of 5.0 and osmolarity of 308 mOsm/L. LR solution has an average pH of 6.5, is hypo-osmolar (272 mOsm/L), and has similar electrolytes (130 mM Na+, 109 mM Cl-, 28 mM lactate, etc.) to plasma.\
2)Inj.
1amp THIAMINE in 100ml NS, TID
- Thiamine
is given in patients that are chronic alcoholics, due to the pathology which
causes the thiamine levels in the body are deficient and thiamine is required
in the breakdown of glucose.
in the above study r
3)Inj.
Lorazepam
Lorazepam
is mostly given to reduce the anxiety the patient feels.
Mechanism
of action: Lorazepam binds to benzodiazepine receptors on the postsynaptic
GABA-A ligand-gated chloride channel neuron at several sites within the central
nervous system (CNS). It enhances the inhibitory effects of GABA, which
increases the conductance of chloride ions into the cell.
Efficacy
study: https://pubmed.ncbi.nlm.nih.gov/6120058/#:~:text=Subjective%20and%20objective%20data%20clearly,(P%20less%20than%200.01).
Subjective and objective data clearly demonstrated that lorazepam was effective for both inducing and maintaining sleep. Sleep latency was reduced from a baseline value of 34.6 min to 17.9 min
4)T.
Pregabalin 75mg/PO/ BD
Mechanism
of action: Pregabalin has demonstrated anticonvulsant, analgesic, and
anxiolytic properties in preclinical models. The drug's exact mechanism of
action is unclear, but it may reduce excitatory neurotransmitter release
by binding to the α2-δ protein subunit of voltage-gated calcium channels.
Indication:
Pregabalin is indicated for the management of neuropathic pain associated with
diabetic peripheral neuropathy, postherpetic neuralgia, fibromyalgia,
neuropathic pain associated with spinal cord injury, and as adjunctive therapy
for the treatment of partial-onset seizures in patients 1 month of age and
older.
CONCLUSIONS—Treatment with pregabalin across its effective dosing range is associated with significant, dose-related improvement in pain in patients with DPN.
5)Lactulose
30ml/PO/BD
Mechanism of action:

Conclusion: Lactulose has significant beneficial effects for patients with MHE compared with placebo or no intervention.
6)Inj
2 ampoule KCl (40mEq) in 10 NS over 4 hours
Mechanism
of action: Supplemental potassium in the form of potassium chloride may be able
to restore normal potassium levels.
Indication:
For use as an electrolyte replenisher and in the treatment of hypokalemia.
efficacy: https://pubmed.ncbi.nlm.nih.gov/2310280/
7)Syp
Potchlor 10ml in one glass water/PO/BD
It is
a supplement potassium and helps in replenishing in cases of hypokalemia
QUESTION: Why have neurological symptoms appeared
this time, that were absent during withdrawal earlier? What could be a possible
cause for this?
The patient
mainly deals with two main neurological symptoms- seizures and memory loss
The process
of repeated alcohol intake and withdrawal is known as kindling. During the
kindling effect, the brain and body become incredibly sensitive to alcohol and the
withdrawal symptoms that occur during cessation. Every relapse and subsequent
detox from alcohol becomes more intense and painful. More severe withdrawal
symptoms can occur because of the kindling effect during each incidence of
relapse and withdrawal. The risk of seizures and a potentially dangerous
condition called delirium tremens increase due to the kindling effect.
Alcohol may have a direct neurotoxic effect on
cortical neurons, but much of the damage may be secondary to a pre-existing
pathology caused by thiamine deficiency.
The continuous
use of alcohol must have resulted in thiamine deficiency which could be causing
neurological symptoms. Previously there must have not been a decrease in levels
of thiamine in a patient and that can be the reason why he never displayed
neurological symptoms before. With increase in alcohol and withdrawal processes
the patient’s thiamine deficiency is now causing neurological symptoms
QUESTION: What is the reason for giving thiamine
in this patient?
-Thiamine
is usually given in patients with this type of presentation because of the
history of alcohol withdrawal and alcohol habituation.
-A
chronic alcoholic has a depleted supply of thiamine in the body which can give
rise to neurological symptoms, such as Wernicke Encephalopathy.
-To
abate some of the symptoms, thiamine is given to replenish the supply of the
patient.
QUESTION: What is the probable reason for kidney
injury in this patient?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6826793/
Both
acute and chronic alcohol consumption can compromise kidney function,
particularly in conjunction with established liver disease. Excessive alcohol
consumption can have profound negative effects on the kidneys and their
function in maintaining the body’s fluid, electrolyte, and acid-base balance,
leaving alcoholic people vulnerable to a host of kidney-related health problems.:
Chronic alcohol consumption induces profound injury in several organs that may
affect and aggravate the effect of ethanol on the kidney. Ethanol itself
markedly induces the expression of the microsomal ethanol oxidation system
(CYP2E1), producing reactive oxygen species as a byproduct. Increased
gastrointestinal permeability and endotoxin load may lead to alcoholic
steatohepatitis resulting in excessive immunoglobulin A (IgA) load. IgA
deposits may accumulate in the kidney, leading to glomerulopathy. Renal
microcirculatory changes in advanced liver cirrhosis leads to hepatorenal
syndrome. Alcohol-induced skeletal muscle damage leads to excessive amounts of
circulating myoglobin, causing renal tubular injury because of increased
oxidative stress. Due to the development of alcoholic cardiomyopathy, chronic
renal hypoxia develops, activating the renin–angiotensin–aldosterone system
(RAAS), which in turn leads to further free radical production and to the
propagation of fibrotic pathways.
Though
there only a few studies which talk about the alcohol’s direct effect on
kidney. Alcohol cause various other imbalances which cause decrease in their
function.
QUESTION: What is the probable cause for the
normocytic anemia?
Kidney
disease is associated with normocytic anemia
QUESTION: Could chronic alcoholism have aggravated
the foot ulcer formation? If yes, how and why?
Similar
to diabetes chronic alcoholism causes a depression in the immune system. This
can aggravate the for ulcer formation. It
can also cause alcoholic neuropathy Alcoholic neuropathy involves coasting
caused by damage to nerves that results from long term excessive drinking of
alcohol and is characterized by spontaneous burning pain, hyperalgesia, and
allodynia. Chronic presentation will increase the chances of foot ulcer
formation and also increase the time of recovery.
CASE: https://kausalyavarma.blogspot.com/2021/05/a-52-year-old-male-with-cerebellar.html?m=1
QUESTION: What is the evolution of the
symptomology in this patient in terms of an event timeline and where is the
anatomical localization for the problem and what is the primary etiology of the
patient’s problem?
Timeline
of the patient is as follows-
|
7
days back |
a
history of giddiness that started around 7 in the morning; subsided upon
taking rest; associated with one episode of vomiting |
|
4
days back |
Patient
consumed alcohol; He developed giddiness that was sudden onset, continuous
and gradually progressive. It increased on standing and while walking. H/O
postural instability- falls while walking Associated
with bilateral hearing loss, aural fullness, presence of tinnitus Associated
vomiting- 2-3 episodes per day, non-projectile, non-bilious without food
particles |
|
Present
day of admission |
Slurring
of speech, deviation of mouth that got resolved the same day |
Anatomical
location- There is a presence of an infarct in the inferior cerebellar
hemisphere of the brain.
Etiology-
Ataxia is the lack of muscle control or co-ordination of voluntary movements,
such as walking or picking up objects. This is usually a result of damage to
the cerebellum. There are many conditions causing ataxia such as head trauma,
alcohol abuse, stroke, tumors, cerebral palsy etc. this patient was diagnosed
with hypertension for which he was prescribed medication but the patient did
not use the medication. This must have caused uncontrolled blood pressure leading
to stroke.
QUESTION: What are the mechanism of action,
indication and efficacy over placebo of each of the pharmacological and non-pharmacological
interventions used for this patient?
ANS.
1)Tab
Vertin 8mg-
This
is an anti-vertigo medication known as betahistine
MOA-Betahistine
has two mechanisms of action. Primarily, it is a weak agonist on the H1 receptors
located on blood vessels in the inner ear. This gives rise to local
vasodilation and increased permeability, which helps to reverse the underlying
problem of endolymphatic hydrops.
More
importantly, betahistine has a powerful antagonistic effects at H3 receptors,
thereby increasing the levels of neurotransmitters histamine, acetylcholine, norepinephrine, serotonin,
and GABA released
from the nerve endings. The increased amounts of histamine released from
histaminergic nerve endings can stimulate receptors
Indications- Prescribed for balance disorders. In this case it is used due to patient’s history of giddiness and balance issues.
2)Tab
Zofer 4mg-
This
is ondanseteron, an anti-emetic
MOA-
It is a 5H3 receptor antagonist on vagal afferents in the gut and they block
receptors even in the CTZ and solitary tract nucleus.
Indications- Used to control the episodes of vomiting and nausea in this patient.
3)Tab
Ecosprin 75mg-
This
is a NSAID(aspirin)
MOA-
They inhibit COX-1 and COX-2 thus decreasing the prostaglandin level and thromboxane
synthesis
Indications-
They are anti platelet medications and in this case used to prevent formation
of blood clots in blood vessels and prevent stroke.
efficacy: https://pubmed.ncbi.nlm.nih.gov/3966266/
40 mg aspirin daily inhibited platelet responses as effectively as higher doses of aspirin in patients who had recent cerebral ischemia and showed a cumulative antiplatelet effect.
4)Tab
Atorvostatin 40mg-
-This
is a statin
MOA-
It is an HMG CoA reductase inhibitor and thus inhibits the rate limiting step
in cholesterol biosynthesis. It decreases blood LDL and VLDL, decreases
cholesterol synthesis, thus increasing LDL receptors in liver and increasing LDL
uptake and degeneration. Hence plasma LDL level decreases.
Indications- Used to treat primary hyperlipidemias. In this case it is used for primary prevention of stroke
efficacy: https://pubmed.ncbi.nlm.nih.gov/17910521/.
atorvastatin has developed a well defined role in the primary and secondary prevention of cerebrovascular disease, and appears to have a particularly prominent place in preventing such disease in CHD patients, and in the post-stroke and post-TIA setting in patients without CHD
5)Clopidogrel
75mg-
-It
is an antiplatelet medication
MOA-
It inhibits ADP mediated platelet aggregation by blocking P2Y12 receptor on the
platelets.
Indications- In this case it decreases the risk of heart disease and stroke by preventing clotting
6)Thiamine-
- It
is vitamin B1
In this case, the patient consumes excess
alcohol which can cause thiamine deficiency causing many neurological disorders.
Indications-
Given to this patient mainly to prevent Wernicke’s encephalopathy- that can
lead to confusion, ataxia and opthalmoplegia.
7)Tab
MVT-
-This
is methyl cobalamin
-given
to the patient for vit b12 deficiency
QUESTION: Did the patients history of DE novo
hypertension contribute to his current condition?
High
blood pressure damages arteries throughout the body, creating conditions where
they can burst or clog more easily. Weakened arteries in the brain, resulting
from high blood pressure, put you at a much higher risk for stroke. high blood
pressure can cause several problems in the brain, including:
Transient
ischemic attack (TIA). Sometimes called a ministroke, a TIA is a
brief, temporary disruption of blood supply to your brain. Hardened arteries or
blood clots caused by high blood pressure can cause TIA. TIA is
often a warning that you're at risk of a full-blown stroke.
Stroke. A
stroke occurs when part of your brain is deprived of oxygen and nutrients,
causing brain cells to die. Blood vessels damaged by high blood pressure can
narrow, rupture or leak. High blood pressure can also cause blood clots to form
in the arteries leading to your brain, blocking blood flow and potentially
causing a stroke.
QUESTION: Does the patient’s history of alcoholism
make him more susceptible to ischemic or hemorrhagic stroke?
According
to a Cambridge study, heavy drinkers have 1.6 more chance of intracerebral hemorrhage
and a 1.8 increased chance of subarachnoid hemorrhage. The adverse effect on BP
that is seen due to increased drinking is a major stroke risk factor and increase
the risk of heart stroke.
Many
studies show that with mild and moderate drinking. the risk of ischemic stroke
decreases due to decreased level of fibrinogen which helps in the formation of
blood clots. However, heavy alcohol intake is associated with impaired
fibrinolysis, increased platelet activation and increased BP and heart rate.
So in
this case, patient’s history of alcoholism, coupled with his hypertension could
be a causative factor of his current condition.
https://www.ahajournals.org/doi/pdf/10.1161/01.STR.19.12.1565
CASE: https://bejugamomnivasguptha.blogspot.com/2021/05/a-45-years-old-female-patient-with.html
QUESTION: 1)
What is the evolution of the symptomatology in this patient in terms of an
event timeline and where is the anatomical localization for the problem and
what is the primary aetiology of the patient's problem?
10 years back –
episode of right and left upper limb paralysis
1 year back:
right and left paresis due to hypokalaemia
8 months ago-
bilateral pedal oedema, gradually progressing, present in both sitting and
standing position, relieved on taking medication
7 months ago –
diagnosed with infection in the blood
2 months ago –
visited our hospital for neck pain and received medication
6 days ago –
pain in the left upper limb, radiating along the upper limb, dragging type,
nocturnal increase in the pain, aggravated during palpitations and relieved on
medication
5 days ago –
palpitations,
sudden in onset, more during night time, aggravated by lifting weights and
speaking continuously, relieved by drinking more water, medication
dyspnoea during
palpitation (NYHA CLASS 3)
chest pain
associated with chest heaviness
the anatomical
location is the cervical spine
the patient
experienced episodes of palpitations, paresis, paralysis and oedema because of hypokalaemia
neck pain is
due to cervical spondylosis
QUESTION: What
are the reasons for recurrence of hypokalaemia in her? Important risk factors
for her hypokalaemia?
ANS) since the
patient complains of oedema the drugs used to relieve it such as diuretics can
cause hypokalaemia
The patient
also no albumin which is a cause for both oedema and hypokalaemia
The risk
factors include-
1.
Alcohol
use(excessive)
2.
Chronic
kidney disease
3.
Diabetic
ketoacidosis
4.
Diuretics
(water retention relievers)
5.
Excessive
laxative use
6.
Folic
acid deficiency
7.
Primary
aldosteronism
8.
Some
antibiotic use
QUESTION: What
are the changes seen in ECG in case of hypokalaemia and associated symptoms?
ANS) The
earliest electrocardiogram (ECG) change associated with hypokalaemia is a
decrease in the T-wave amplitude. As potassium levels decline further,
ST-segment depression and T-wave inversions are seen, while the PR interval can
be prolonged along with an increase in the amplitude of the P wave. The U
wave is described as a positive deflection after the T wave, often best seen in
the mid-precordial leads

CASE: https://rishikoundinya.blogspot.com/2021/05/55years-old-patient-with-seizures.html
QUESTION: Is there any relationship between
occurrence of seizure to brain stroke. If yes, what is the mechanism behind it?
-stroke
is one of the most common cause of seizures in the elderly.
post seizure stroke is of 2 types:
Early onset
seizures have peak within 24 hours after stroke.
Late onset
seizures occur after 2 week of stroke onset, peak within 6-12 months after the stroke,
has a higher rate of recurrence
PATHOGENESIS OF
SEIZURES FOLLOWING STROKE-
There
are several causes for early onset seizures after ischaemic strokes. An
increase in intracellular Ca2+ and Na+ with a resultant lower
threshold for depolarisation, glutamate excitotoxicity, hypoxia, metabolic
dysfunction, global hypo perfusion, and hyper perfusion injury (particularly
after carotid end arterectomy) have all been postulated as putative
neurofunctional aetiologies. Seizures after haemorrhagic strokes are thought to
be attributable to irritation caused by products of blood metabolism. The exact
pathophysiology is unclear, but an associated ischaemic area secondary to
haemorrhage is thought to play a part. Late onset seizures are associated with
the persistent changes in neuronal excitability and gliotic scarring is most
probably the underlying cause. Hemosiderin deposits are thought to cause
irritability after a haemorrhagic stroke.In
childhood, post‐stroke
seizures can occur as part of perinatal birth trauma.
QUESTION: In the previous episodes of seizures,
patient didn't lose his consciousness but in the recent episode he lost his consciousness
what might be the reason?
The patient has
a history of seizure activity, causing increased mechanical and chemical
activity in the brain, which can lead to the development of organic lesions in
the brain. The size of the lesion is directly proportional to the severity of
the symptoms.
This patient
has a history of recurrent seizures- 15 episodes in the last 5 years
There might be
an aggravation of his symptoms during this episode when compared to the
previous episodes. This severity could be the cause for his loss of consciousness.
CASE: https://nikhilasampathkumar.blogspot.com/2021/05/a-48-year-old-male-with-seizures-and.html?m=1
QUESTION: What could have been the reason for the
patient for developing ataxia in the past 1 year?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4492805/
The
patient has a history of alcohol consumption in excess the past three years. Excessive
alcohol consumption is a risk factor for development of cerebellar dysfunction
or cerebellar ataxia.
The
alteration in GABAA receptor-dependent neurotransmission is a potential
mechanism for ethanol-induced cerebellar dysfunction. Recent advances indicate
ethanol-induced increases in GABA release are not only in Purkinje cells (PCs),
but also in molecular layer interneurons and granule cells. Ethanol is shown to
disrupt the molecular events at the mossy fiber – granule cell – Golgi cell
(MGG) synaptic site and granule cell parallel fibers – PCs (GPP) synaptic site,
which may be responsible for ethanol-induced cerebellar ataxia. Aging and
ethanol may affect the smooth endoplasmic reticulum (SER) of PC dendrites and
cause dendritic regression. Ethanol withdrawal causes mitochondrial damage and
aberrant gene modifications in the cerebellum. The interaction between these
events may result in neuronal degeneration, thereby contributing to motoric
deficit. Ethanol activates double-stranded RNA (dsRNA)-activated protein kinase
(PKR) and PKR activation is involved ethanol-induced neuroinflammation and
neurotoxicity in the developing cerebellum. Ethanol alters the development of
cerebellar circuitry following the loss of PCs, which could result in
modifications of the structure and function of other brain regions that receive
cerebellar inputs. Lastly, choline, an essential nutrient is evaluated for its
potential protection against ethanol-induced cerebellar damages. Choline is
shown to ameliorate ethanol-induced cerebellar dysfunction when given before
ethanol exposure.
QUESTION: What was the reason for his IC bleed?
Does alcoholism contribute to bleeding diathesis?
https://pubs.niaaa.nih.gov/publications/arh21-1/42.pdf
as
mentioned this patient has a history of excessive alcohol consumption. Alcohol causes
various hematological complications as described in the study above.
Bleeding
diathesis is an unusual susceptibility to bleed (hemorrhage) mainly due to
hypercoagulability. Heavy drinking can cause thrombocytopenia, as well as
impact shape and functions of platelets. Impaired platelet function, together
with reduced platelet count, can contribute to this condition associated with
chronic alcoholism. This can also cause an increased incidence and recurrence
of gastrointestinal hemorrhage associated with excessive alcohol intake
Another
study conducted by Cambridge indicates, heavy drinkers have 1.6 more chance of
intracerebral hemorrhage and a 1.8 increased chance of subarachnoid hemorrhage
QUESTION: Does the patient’s history of road traffic
accident have any role in his present condition?
ANS:
https://www.ahajournals.org/doi/pdf/10.1161/01.STR.14.4.617
The
above study is similar to the case discussed where an accident occurring years
ago has eventually led to an infarct.
Similarly,
the accident that occurred in our patient 4 years ago can be the reason for his
present condition.
QUESTION: What are warning signs of CVA?
- Sudden numbness or
weakness in the face, arm, or leg, especially on one side of the body.
- Sudden confusion,
trouble speaking, or difficulty understanding speech.
- Sudden trouble
seeing in one or both eyes.
- Sudden trouble
walking, dizziness, loss of balance, or lack of coordination.
- Sudden severe
headache with no known cause.
QUESTION: What is the drug rationale in CVA?
1)thrombolysis- The NINDS rtPA Stroke
Study compared the use of intravenous rtPA given within three hours after
stroke onset versus placebo [21]. The rtPA-treated group showed a significant neurological
improvement when compared to the untreated group.
Therapy with
rtPA is given at a dose of 0.9 mg/kg IV without exceeding a maximum dose of 90
mg with 10% given as a loading bolus over 1 minute and the remainder as an
infusion over 60 minutes. During the infusion and for one hour after concluding
the infusion, the patient’s vital signs should be monitored and neurological
assessment done every 15 minutes. Thereafter, observations should be carried
out every 30 min for the next 6 hours and hourly afterward until 24 hours have
transpired since treatment.
2)antiplatelet Therapy-Due
to the thrombotic origin of AIS and the involvement of platelet aggregation in
the development of said thrombus, antiplatelet drugs play an obvious and
pivotal role in the medical treatment. Perhaps the most widely used
antiplatelet agent is non-steroidal anti-inflammatory drugs (NSAID)
acetylsalicylic acid (aspirin)
Aspirin at low doses binds and inhibits the platelet COX-1
irreversibly and consequently impairs the production of prostaglandins and thromboxane’s,
noting thromboxane A2 (TXA2) in particular. The absence of TXA2 leads
to the reduction in the TXA2-mediated amplification of platelet activation and
thus hinders the platelet aggregation phenotype that includes morphological changes
and expression of the fibrinogen receptor necessary for platelet aggregation.
3.
Anticoagulant therapy
Anticoagulants
are a heterogeneous group of pharmacological agents that by interacting with
the coagulation cascade disrupt the formation of the fibrin mesh that forms the
scaffold of the clot. When in homeostasis, the blood elements that participate
in this process are kept at check thus preventing the formation of a blood
clot in situ, or thrombus, inside the blood
vessels.
CASE: https://amishajaiswal03eloggm.blogspot.com/2021/05/a-50-year-old-patient-with-cervical.html
QUESTION: What is myelopathy hand?
https://pubmed.ncbi.nlm.nih.gov/3818752/
https://online.boneandjoint.org.uk/doi/abs/10.1302/0301-620X.69B2.3818752
A characteristic
dysfunction of the hand has been observed in various cervical spinal disorders.
These are termed as myelopathy hand and appear to be due to pyramidal tract
involvement. There is loss of power of adduction and extension of the ulnar
fingers and inability to grip and release rapidly with these fingers.
QUESTION: What is finger escape?
finger escape
sign is a component of WARTENBERG’S SIGN.
it is one of
the signs in cervical cord damage particularly cervical myelopathy
When a patient
holds fingers extended and adducted, the small finger spontaneously adducts
indicating a weakness of intrinsic muscle. This commonly results from weakness
of the ulnar nerve innervated intrinsic hand muscles.
QUESTION: What is Hoffman’s reflex?
Also known as
DIGITAL reflex, SNAPPING reflex, JACOBSON’S reflex.
. It is used to
examine the reflexes of upper extremities.
Hoffman’s
reflex is a neurological examination finding elicited by a reflex test which
can help verify the presence or absence of issues arising from the
corticospinal tract.
Procedure: The
Hoffmann's reflex test itself involves loosely holding the middle finger and
flicking the fingernail downward, allowing the middle finger to flick upward
reflexively. A positive response is seen when there is flexion and adduction of
the thumb on the same hand
INTERPRETATION: If
there is no movement in the index finger or thumb after this motion, the person
has a negative Hoffman’s sign. If the index finger and thumb move, the
person has a positive Hoffman’s sign.
A positive
Hoffman sign indicates an upper motor neuron lesion and corticospinal pathway
dysfunction likely due to cervical cord compression. (ex: CERVICAL MYELOPATHY)
However, a
positive Hoffman sign can be present in an entirely normal patient. This
happens in individuals who are hyper reflexive.
CASE: https://neerajareddysingur.blogspot.com/2021/05/general-medicine-case-discussion.html?m=1
QUESTION: What can be the cause of her condition?
The patient’s GTCS episodes
can be due to acute
cortical vein thrombosis as seen in her MRI.
Seizures are
the most common symptoms of CVT.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5771304/
this case report illustrates that CVT can occur in the
setting of anaemia and thrombocytopenia.
the above case
is similar to our patient. Though neurological manifestations are not common in
iron deficiency anaemia our patient presented with CVT. Also, our patient had thrombocytopenia which one would have
expected to cause a bleeding tendency but paradoxically could have contributed
to the development of the venous thrombosis as explained in the article above.
The associated symptoms such as headache and vomiting can be
explained by the midline shift.
QUESTION: What are the risk factors for cortical
vein thrombosis?
· - birth control or excess oestrogen use.
· - dehydration.
· -ear, face, or neck infection.
· -protein deficiencies.
· -head trauma or injury.
· -obesity.
· -cancer.
· -tumour.
QUESTION: There was seizure free period in between but
again sudden episode of GTCS why? Resolved spontaneously why?
The patient developed high
grade fever (the patient had thrombophlebitis) with could have been the cause
of the seizures. The decrease in the fever could have resolved the seizures.
QUESTION: What drug was used in suspicion of cortical venous sinus
thrombosis?
The approach to treatment includes
anticoagulation (intravenous heparin or subcutaneous low molecular weight
heparin), thrombolysis (systemic or local), and symptomatic treatment (including
antiepileptic therapy, lowering intracranial pressure, decompressive craniotomy)
SYSTEM: CARDIOLOGY
CASE: https://muskaangoyal.blogspot.com/2021/05/a-78year-old-male-with-shortness-of.html
QUESTION:What is the difference btw heart failure
with preserved ejection fraction and with reduced ejection fraction?
Ejection fraction
is expressed as a percentage for measuring how much blood the left ventricle
pumps out with each contraction.
-HF with
reduced ejection fraction(HFrEF) is also known as systolic heart failure.
in this there
is no adequate chamber dilatation as the heart muscle is unable to contract. Therefore,
expels less oxygen rich blood into the body. Patients will have lower than normal
left ventricular ejection fraction.
Causes:
diabetes, valvular heart disease etc.
-HF with preserved
ejection fraction(HFpEF) is also known as diastolic HF. In this the muscles of
the heart contract normally and the heart pumps a normal amount of blood that
enters it. There is heart muscle thickening which may cause the ventricle to
hold small amount of blood. Therefore, the hearts output is normal but its
limited capacity is inadequate to meet the body’s requirement.
Causes:
hypertrophic cardiomyopathy, aortic stenosis, CAD, high blood pressure
QUESTION: Why haven't we done pericardiocenetis in
this patient?
Pericardiocenetis
is a procedure done to remove fluid that has built up in the pericardium. This process
requires a lot of precision as it can lead to a damage in the surrounding
pleura. The patient has mild-moderate pericardial effusion, for which he was
given symptomatic treatment rather than an invasive procedure like
pericardiocenetis. The patient also has pleural effusion which can make the
process difficult. Taking the patients state into account an invasive therapy
that might cause damage was avoided.
QUESTION: What are the risk factors for
development of heart failure in the patient?
The patient has
the following risk factors:
the patient is
a chronic alcoholic- 90ml/day for the last 30 years
chronic
alcoholism is a major risk factor towards developing alcoholic cardiomyopathy.
The patient is
a chronic smoker-30 years
Cigarette smoking
can cause vascular changes and also directly effects the myocardium through
increased oxidative stress and activated inflammatory pathways leading to
systolic and diastolic dysfunction.
The patient is
diabetic:
Diabetes can
eventually cause damage to vessels and nerves supplying the heart along with
having certain effects on myocardial structure and function increasing the risk
of heart failure.
The patient has
hypertension:
Hypertension increases
the load on the heart muscles causing hypertrophy which can lead to a heart
failure
The patient was
diagnosed with first degree AV block
This is
associated with increased risk of heart failure.
QUESTION: What could be the cause for hypotension
in this patient?
The patient is using a diuretic called LASIX and
a hypertension drug telmasaratn, along with pericardial effusion. The fluid
around the heart is effecting its pumping ability (decreased) along with this
the diuretic and telmasartan are further causing a decrease in the pressure
which has led to hypovolemia and thereby hypotension
Hypotension in
this patient could be due to combination of pericardial effusion and use of
diuretic LASIX.
The pumping
ability of the heart in this patient is compromised, along with this he is on
Diuretic and anti-hypertensive (Telma 40 mg), fluid restriction- all this might
result in Hypovolemia and thereby Hypotension.
CASE: https://muskaangoyal.blogspot.com/2021/05/a-73-year-old-male-patient-with-pedal.html
QUESTION: What are the possible causes for heart failure
in this patient?
the patient has various
comorbidities which could have led to a heart failure
1.
The
patient was diagnosed with type 2 diabetes mellitus 30 years ago and has been
taking human mixtrad insulin daily and was also diagnosed with diabetic
triopathy indicating uncontrolled diabetes which is major risk factor for heart
failure
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5494155/
2.
The
patient was also diagnosed with hypertension 19 yrs. ago which is also a risk
factor for heart failure
https://pubmed.ncbi.nlm.nih.gov/31472888/
3.
He
is a chronic alcoholic since 40 years which is a risk factor towards heart
failure
https://www.nmcd-journal.com/article/S0939-4753(19)30360-6/fulltext
The
findings in this article provide longitudinal evidence that moderate and heavy
alcohol consumption are associated with decreased LVEF and trend towards a
higher risk of incident LV systolic dysfunction, compared to light drinkers.
4.
The
patient has elevated creatinine and AST/ALT ratios is >2 and was diagnosed with
chronic kidney disease stage IV. CKD is also one of the risk factors for heart
failure
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2900793/
QUESTION:
what is the reason for anaemia in this case?
The
patient has normocytic normochromic anaemia. it could be anaemia of a chronic
disease as the patient is diagnosed with CKD stage IV.
Chronic
kidney disease results in decreased production of erythropoietin which in turn
decreases the production of red blood cells from the bone marrow.
Patient’s
with anaemia and CKD also tend to have deficiency in nutrients like iron,
vitamin B12 and folic acid essential in making healthy red blood cells
QUESTION: What is the reason for blebs and non-healing
ulcer in the legs of this patient?
The most
common cause for blebs and non-healing ulcer in this patient is diabetes
mellitus. CKD is also known to cause delay in healing of wounds along with
poorly controlled diabetes. Anaemia can also slow down the process of healing
due to low oxygen levels.
QUESTION: What sequence of stages of diabetes has been noted in this
patient?
There are 4 stages in type 2 diabetes- insulin
resistance, prediabetes, type 2 diabetes and type 2 diabetes and vascular complications, including
retinopathy, nephropathy or neuropathy and, or, related microvascular events.
The patient is diagnosed with diabetic
triopathy exhibiting sequence of neuropathy, retinopathy and nephropathy
The patient has been diagnosed with diabetic retinopathy, CKD stage IV and shows signs of diabetic neuropathy such as numbness
CASE: https://preityarlagadda.blogspot.com/2021/05/biatrial-thrombus-in-52yr-old-male.html
QUESTION: What is the evolution of the
symptomology in this patient in terms of an event timeline and where is the
anatomical localization for the problem and what is the primary etiology of the
patient’s problem?
ANS.
Timeline of the patient is as follows-
|
1 year ago |
shortness of
breath (Grade II- SOB on exertion); He visited the hospital where he was
diagnosed to be hypertensive (on medication |
|
2 days ago |
Shortness of
breath Grade II (on exertion) which progressed to Grade IV (at rest) for
which he visited local RMP and was referred to our hospital. Patient also
complains of decreased urine output since 2 days.
|
|
Present day |
SOB grade IV
(on rest) and anuria for the past one day.
|
Anatomical
Location- the cardiac region.
Etiology-
Congestive heart failure is a chronic progressive condition that affects the
pumping power of the cardiac muscle. It occurs if the heart cannot pump
(systolic) or fill (diastolic) adequately. Loss of atrial contraction and left
atrial dilation in this case cause stasis of blood in the left atrium and may
lead to thrombus formation in the left atrial appendage. This predisposes to
stroke and other forms of systemic embolism.
QUESTION: What are the mechanism of action,
indication and efficacy over placebo of each of the pharmacological and non-pharmacological
interventions used for this patient?
1)INJ.
Dobutamine-
Mechanism
of action- It is a synthetic catecholamine, that acts on B1, B2 and alpha 1 receptor.
Indications-
It is a potent inotropic agent but only causes a slight increase in heart rate.
It is given to patients with acute heart failure as iv infusion.
Efficacy: https://www.ncbi.nlm.nih.gov/books/NBK470431/
While the drug is safe, its use requires close monitoring as it has the potential to raise blood pressure and heart rate severely. Overall, the effects of dobutamine are short-lived. As soon as the infusion stops, the hemodynamic parameters will reverse.
2)TAB.
Digoxin-
Mechanism
of action- It acts on the digitalis receptor and inhibits NA-K-ATPase,
increasing cardiac output.
Indications-
Digitalis is used in patients with low output failure especially when
associated with atrial fibrillation, as indicated in this case.
Efficacy: https://pubmed.ncbi.nlm.nih.gov/26913372/
3)INJ.
Unfractionated Heparin 5000-
Mechanism
of action- At low concentration, heparin selectively inhibits the conversion of
prothrombin to thrombin, thus preventing thrombus formation. High dose heparin
has antiplatelet action and prolongs bleeding time.
Indications-
Patient had a biatrial thrombus and it was used to prevent further thrombus
formation.
Efficacy:https://pubmed.ncbi.nlm.nih.gov/2882339/
according to the study: Low-dose heparin appears to be effective, safe, well tolerated, and free from haemorrhagic risk for the prevention of myocardial reinfarction.
4)TAB.
Carvedilol 3.125mg BD
Indications- Used as a long term drug to
reduce mortality in patients with congestive heart failure.
5)TAB.
Acetyl cysteine 600mg PO TID
6)TAB.
Acitrom 2mg OD
Mechanism
of action- It is an anticoagulant that functions as a vitamin K antagonist.
Indications-
oral anticoagulant which helps to prevent formation of harmful blood clots in
the legs, lungs, brain and heart. It is used for deep vein thrombosis,
pulmonary embolism and stroke prevention.
7)TAB. Cardivas 3.125mg PO/BD
Mechanism
of action- It is carvedilol. It blocks B1, B2, Alpha 1 adrenergic receptors and
no intrinsic sympathomimetic activity.
Indications-
Used as a long term drug to reduce mortality in patients with congestive heart
failure.
8)TAB.
Dytor 10mg PO/OD
Mechanism
of action- It is torsemide, a loop high ceiling diuretic. It acts on the thick
ascending limb of the loop of Henle, increases Na, K and Cl excretion in the
urine.
Indications-
preferred in cases of hypertension associated with CCF and renal failure.
9)TAB
Pan D 40mg PO/OD
Mechanism
of action- It is a combination of domperidone and pantoprazole. It is a proton
pump inhibitor and helps decrease acid production in the stomach.
Indications-
used to treat gastroesophageal reflux disease (Acid reflux) and peptic ulcer
disease by relieving the symptoms of acidity such as indigestion, heartburn,
stomach pain, or irritation.
10)TAB.
Taxim 200mg PO/OD
Mechanism
of action- It is cefixime. They are beta-lactam antibiotics that inhibit
synthesis of bacterial cell wall and produce a bactericidal effect.
Indications-
Given mainly to prevent development of bacterial infections.
11)INJ.
Thiamine 100mg in 50ml NS IV/TID
It
is vitamin B1. It is naturally found in many foods in the human diet. In this
case, the patient consumes excess alcohol- so he may get thiamine deficiency
due to poor nutrition and lack of essential vitamins due to impaired ability of
the body to absorb these vitamins.
12)INJ.
HAI S.C 8U-8U-6U
Insulin
given in this case to treat the patients DE novo diabetes mellitus.
QUESTION: What is the pathogenesis of renal
involvement due to heart failure (cardio renal syndrome)? Which type of cardio
renal syndrome is this patient?
https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000000664
Cardio
renal syndrome encompasses a spectrum of disorders involving both the heart and
kidneys in which acute or chronic dysfunction in 1 organ may induce acute or
chronic dysfunction in the other organ. It represents the confluence of
heart-kidney interactions across several interfaces. These include the
hemodynamic cross-talk between the failing heart and the response of the
kidneys and vice versa, as well as alterations in neurohormonal markers and
inflammatory molecular signatures characteristic of its clinical phenotypes. There
is immediate stress on the kidney through pathophysiological connections when
CHF develops. The connectivity of the vascular bed, and its regulation by the
sympathetic nervous system (SNS) and renin-angiotensin-aldosterone system
(RAAS), continues the stress on the nephron. The long-term process results in
scarring and fibrosis to both organs.
CHF as a syndrome occurs due to the over
expression of biologically active molecules that are capable of deleterious
effects. The cells such as the myocardial myocytes, are capable of producing
these potentially toxic effectors within close vicinity of the injury with the
capacity for ongoing autocrine and paracrine activity. The spillover of this
toxic milieu reaches the kidney, which has to regulate salt and water retention
to compensate for loss of cardiac output. Finally, an important source of renal
stress is increased cardiac preload.
The
kidneys receive 25% of blood flow, where the majority goes to the cortex, which
also has the greatest neural innervations to regulate changes acutely. The
medulla receives only 10% of the blood supply. The renal microvascular bed
however is continuous throughout. Thus, disease in any glomeruli could have
implications when placed under supraphysiological stress from SNS or RAAS and
matched with early disease in vascular endothelium and nitric oxide systems.
Compensation
to ensure adequate GFR includes increased renal blood flow (afferent arteriolar
vasodilatation), filtration pressure (via efferent arteriolar vasoconstriction)
and glomerular hypertrophy, and hyper filtration (leads to scarring).
In
this case the patient has Type 4 cardio renal syndrome: a chronic decline in
kidney function that results in chronic cardiac dysfunction.
QUESTION: What are the risk factors for
atherosclerosis in this patient?
ANS.
In this case, the risk factors for the development of atherosclerosis include:
-Patient
has Diabetes mellitus type 2
diabetes can accelerate atherosclerosis by
driving inflammation and slowing down blood flow.
-Patient
has history of alcohol abuse
it can lead to atherosclerosis and increase
the risk of stroke.
-Patient
has a history of NSAID abuse
which can change the vessels ability to relax
and also stimulate growth of smooth muscle cells inside the arteries, thus
leading to the clogging of the arteries.
-Patient
also has a history of hypertension
effect on the arterial wall also results in
the aggravation and acceleration of atherosclerosis, particularly of the
coronary and cerebral vessels. Moreover, hypertension appears to
increase the susceptibility of the small and large arteries
to atherosclerosis.
QUESTION: Why was the patient asked to get
those APTT, INR tests for review?
ANS.
APTT- Activated partial thromboplastin time; this is a blood test that
characterizes coagulation of blood. The patient has a propensity for thrombus
formation, which needs to be monitored by keeping check on the aPTT levels
which is an indicator for the coagulability of the blood.
INR-
It is international normalized ratio; it is also a measure of the ability of
the blood to clot. This is an important test for patients who are on blood
thinners (i.e.) anticoagulants. The patient in this case was taking heparin, so
everyday reports of his INR value were needed.
TIMELINE OF
EVENTS-
|
12 YEARS AGO |
Diagnosed with
diabetes and the patient is on medication ever since |
|
ONE YEAR AGO |
Heart burn
like episodes since 1 year and relieved without medication |
|
7 MONTHS AGO |
Diagnosed with
pulmonary TB completed full course of treated, presently sputum negative |
|
6 MONTHS AGO |
Diagnosed with
hypertension, is on medication |
|
HALF AN HOUR AGO |
SOB since
half an hour |
Anatomical
localisation - Cardiovascular system
Aetiology:
The patient is both Hypertensive and diabetic, both these conditions can cause
Atherosclerosis: there is build-up of fatty and fibrous material inside the
wall of arteries. (PLAQUE)
QUESTION: What are mechanism of action,
indication and efficacy over placebo of each of the pharmacological and non-pharmacological
interventions used for this patient?
Pharmacological
interventions:
1)TAB MET XL 25
MG/STAT-
contains Metoprolol as active ingredient
MOA:
METOPROLOL is a cardio selective beta blocker
Beta
blockers work by blocking the effects of the hormone epinephrine, also known as
adrenaline. Beta blockers cause your heart to beat more slowly (negative
chronotropic effect)
and with less force
(negative inotropic effect). Beta blockers also help open up your veins and
arteries to improve blood flow.
Indications: it
is used to treat Angina, High blood pressure and to lower the risk of heart attacks.
2)Non
pharmacological intervention advised to this patient is: PERCUTANEOUS CORONARY INTERVENTION.
Percutaneous
Coronary Intervention is a non-surgical procedure that uses a catheter (a
thin flexible tube) to place a small structure called a stent to open up blood
vessels in the heart that have been narrowed by plaque build-up (atherosclerosis).
QUESTION: What are the indications and
contraindications for PCI?
INDICATIONS:
- Acute
ST-elevation myocardial infarction (STEMI)
- Non–ST-elevation
acute coronary syndrome (NSTE-ACS)
- Unstable
angina.
- Stable
angina.
- Anginal
equivalent (e.g., dyspnoea, arrhythmia, or dizziness or syncope)
-High risk
stress test findings.
CONTRAINDICATIONS:
- Intolerance
for oral antiplatelet long-term.
-Absence of
cardiac surgery backup.
-Hypercoagulable
state.
-High-grade
chronic kidney disease.
-Chronic total
occlusion of SVG.
-An artery with
a diameter of <1.5 mm.
QUESTION: What happens if a PCI is performed in a
patient who does not need it? What are the harms of overtreatment and why is
research on over testing and overtreatment important to current healthcare
systems?
Although PCI is
generally a safe procedure, it might cause serious certain complications like
A) Bleeding
B) Blood vessel
damage
C) Allergic
reaction to the contrast dye used
D) Arrhythmias
E) Need for
emergency coronary artery bypass grafting.
Because of all
these complications it is better to avoid PCI in patients who do not require
it.
Research on over
testing and overtreatment is important as they can be more harmful than useful
in many conditions. Such as:
Harms to patients
. Performing
screening tests in patients with who at low risk for the disease which is being
screened.
For example:
Breast Cancer Screenings Can Cause More Harm Than Good in Women Who Are at Low
Risk. A harmless lump or bump could incorrectly come up as cancer during
routine breast screenings. This means that some women undergo surgery,
chemotherapy or radiation for cancer that was never there in the first place.
. Overuse of
imaging techniques such as X- RAYS AND CT SCANS as a part of routine
investigations.
Overuse
of imaging can lead to a diagnosis of a condition that would have otherwise
remained irrelevant - OVER-DIAGNOSIS.
Also the
adverse effects due to this are more when compared to the benefits.
. Over-diagnosis
through over testing can psychologically harm the patient.
Hospitalisations
for those with chronic conditions who could be treated as outpatients [ can
lead to economic burden and a feeling of isolation.
Harm to health care
systems
The use of
expensive technologies and machineries are causing economic burden on health
care systems.
CASE: https://bhavaniv.blogspot.com/2021/05/case-discussion-on-myocardial-infarction.html?m=1
QUESTION: What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
|
3 days ago |
Developed
chest pain on the right side of the chest. |
Anatomical
Localization: Cardiovascular system – Occlusion of the right coronary artery.
Etiology:
Atherosclerosis
– Also known as coronary artery disease, this condition is the most common
cause of heart attacks and occurs when the buildup of fat, cholesterol, and
other substances forms plaque on the walls of the coronary arteries
Coronary
artery spasm – A rare cause of blockage, spasms of the coronary arteries can
cause them to become temporarily constricted.
Coronary
artery tear – Also known as a spontaneous coronary artery dissection, a tear in
a coronary artery can prevent blood from reaching the heart and cause a heart
attack.
QUESTION: What are mechanism of action, indication
and efficacy over placebo of each of the pharmacological and non
pharmacological interventions used for this patient?
TAB.
ASPIRIN 325 mg PO/STAT
-MECHANISM
OF ACTION- Aspirin is a NSAID. They inhibit COX-1 and COX-2 thus decreasing the
prostaglandin level and thromboxane synthesis.
-Indications-
They are anti platelet medications and, in this case, used to prevent formation
of blood clots in blood vessels.
-Efficacy
over Placebo: According to the study, there was a clear reduction in some
serious cardiovascular adverse events. Aspirin use was associated with a
lower risk of myocardial infarction than placebo use or no treatment (risk
ratio [RR], 0.83, 95% confidence interval [CI]: 0.73–0.95, P = 0.005).
TAB
ATORVAS 80mg PO/STAT
--MECHANISM
OF ACTION: Atorvastatin is a statin medication and a competitive inhibitor of
the enzyme HMG-CoA reductase, which catalyzes the conversion of HMG-CoA to
mevalonate, an early rate-limiting step in cholesterol
biosynthesis. Atorvastatin acts primarily in the liver, where decreased
hepatic cholesterol concentrations stimulate the upregulation of hepatic
low-density lipoprotein receptors, which increases hepatic uptake of LDL.
Atorvastatin also reduces Very-Low-Density Lipoprotein-Cholesterol, serum
triglycerides and Intermediate Density, but increases High-Density Lipoprotein
Cholesterol. In vitro and in vivo animal studies also
demonstrate that atorvastatin exerts protective effects independent of its
lipid-lowering properties, also known as the pleiotropic effects of statins.
These effects include improvement in endothelial function, enhanced stability
of atherosclerotic plaques, reduced oxidative stress and inflammation, and
inhibition of the thrombogenic response. Statins were also found to bind
allosterically to β2 integrin function-associated antigen-1, which plays an
essential role in leukocyte movement and T cell activation.
-Indication:
Atorvastatin is indicated for the treatment of several types of dyslipidemias.
Dyslipidemia describes an elevation of plasma cholesterol, triglycerides or
both as well as to the presence of low levels of high-density lipoprotein. This
condition represents an increased risk for the development of atherosclerosis.
Atorvastatin is indicated, in combination with dietary modifications, to
prevent cardiovascular events in patients with cardiac risk factors and/or
abnormal lipid profiles. Atorvastatin can be used as a preventive agent for
myocardial infarction, stroke, and angina, in patients without coronary heart
disease but with multiple risk factors and in patients with type 2 diabetes
without coronary heart disease but multiple risk factors. Atorvastatin may be
used as a preventive agent for non-fatal myocardial infarction, fatal and
non-fatal stroke, revascularization procedures, hospitalization for congestive
heart failure and angina in patients with coronary heart disease.
-Efficacy
over Placebo: Out of 18 studies done, statins were shown to help in 16 studies.
The studies show a 27% reduction in the onset of MI.
TAB CLOPIBB 300mg PO/STAT
-MECHANISM
OF ACTION- Clopidogrel is metabolized to its active form by carboxylesterase-1.3 The
active form is a platelet inhibitor that irreversibly binds to P2Y12 ADP
receptors on platelets. This binding prevents ADP binding to P2Y12 receptors,
activation of the glycoprotein GPIIb/IIIa complex, and platelet aggregation.
-Indications-
Clopidogrel is indicated to reduce the risk of myocardial infarction for
patients with non-ST elevated acute coronary syndrome, patients with
ST-elevated myocardial infarction, and in recent MI, stroke, or established
peripheral arterial disease.
QUESTION: Did the secondary PTCA do any good to the
patient or was it unnecessary?
-
PTCA is known to improve the patient’s vessel patency if it is done within 4
hours of the symptom onset or if it is used as adjunctive therapy along with
some systemic thrombolytic therapy. It can restore up to 90% of the vessel’s
natural state if implemented within enough time.
-Though
there are certain benefits from PTCA, there are some disadvantages too. If done
along with systemic thrombolytics then it can lead to a higher incidence of
bleeding complications. Just PTCA alone, has not proven to show any ventricular
function improvement or decreased mortality.
CASE: https://kattekolasathwik.blogspot.com/2021/05/a-case-of-cardiogenic-shock.h
QUESTION: How did the patient get relieved from his shortness of breath after i.v fluids administration by rural medical practitioner?
-
Rapid breathing along with other presentations like cold, clammy extremities is
an indicator of cardiogenic shock.
-In
cardiogenic shock, there is hypovolemia, which will reduce perfusion to major
organs in the body. when there is decreased perfusion, the body slows starts
shutting down. To halt this process, iv fluids are given rapidly to continue
the perfusion of fluids at the normal rate.
-When
this patient was given fluids, the perfusion returns to normal which helps
abate the shortness of breath.
QUESTION: What is the rationale of using
torsemide in this patient?
- In
patients who have cardio renal syndrome, there is a renal dysfunction along
with cardiac abnormalities. In such patients there is a volume overload and
heart failure, the combination of increased pulmonary artery or central venous
pressure with low systemic pressure may lead to a severe compromise of the net
renal perfusion pressure.
-
Furosemide is a commonly used diuretic to treat volume overload state in heart
failure, yet it is particularly prone to the problem of diuretic resistance
because of its particular pharmacokinetics.
Unfortunately,
chronic diuretic use also induces hypertrophy in distal tubular cells, leading
again to enhanced sodium reuptake, contributing further to diuretic resistance.
Alternatives to furosemide, such as torsemide, have been shown to have a slight
advantage in selected studies because of somewhat more favorable
pharmacokinetics.
QUESTION: Was the rationale for administration of
ceftriaxone? Was it prophylactic or for the treatment of UTI?
-
Patients with cardio renal syndrome are known to have systemic inflammation
which can be drawn parallel to end stage kidney disease. Here there is an
inflammation of monocytes and other inflammatory cells. This puts the patient
in an immune suppressive state.
-Due
to this state, do reduce the chances of infection, as a prophylactic measure,
ceftriaxone might have been started.
SYSTEM: GASTROENTROLOGY
CASE: https://63konakanchihyndavi.blogspot.com/2021/05/case-discussion-on-pancreatitis-with.html
QUESTION: What is the evolution of the
symptomatology in this patient in terms of an event timeline and where is the
anatomical localization for the problem and what is the primary aetiology of
the patient's problem?
TIMELINE OF THE
PATIENT:
|
5YEARS AGO |
An episode of
pain abdomen and vomiting. Treated conservatively at a local hospital. Stopped
alcohol consumption. Symptom free for almost 3 YEARS . Patient
started consuming alcohol, this lead to recurrent episodes of pain abdomen
and vomiting.
|
|
1 YEAR AGO |
5-6 episodes of pain abdomen and vomiting. Treated
by a RMP.
|
|
1 WEEK AGO |
Binge of
alcohol, following this he had pain abdomen and vomiting |
|
SINCE 4 DAYS |
High grade
fever with chills and rigors. Developed constipation Burning
MICTURITION associated with suprapubic pain, increased frequency and urgency.
|
Anatomical
localisation- GASTROINTESTINAL SYSTEM. (stomach and pancreas)
Aetiology:
the patient is a chronic alcoholic, episodes of abdominal pain and vomiting are
following alcohol consumption. therefore, it is heavy drinking that has led to
the above condition in the patient.
QUESTION: What is the efficacy of drugs used
along with other non-pharmacological treatment modalities and how would you
approach this patient as a treating physician?
Drugs used in
this patient -
1) ING. MEROPENEM;
TID for 7 days
. Meropenem is
a broad spectrum carbipenem antibiotic used to treat abdominal and skin
infections.
Mechanism of
action: Meropenem is bactericidal except against Listeria monocytogenes,
where it is bacteriostatic. It inhibits bacterial cell wall synthesis like
other β-lactam antibiotics. In contrast to other beta-lactams, it is highly
resistant to degradation by β-lactamases or cephalosporinases.
BASED ON A
STUDY-In patients with moderate to severe intra-abdominal infections, empirical
monotherapy with meropenem achieved clinical response rates ranging from 91 to
100% in 7 randomised comparative trials. Meropenem also achieved clinical
response rates of over 80% in patients with severe intra-abdominal infections.
2) ING.
METROGYL 500 mg IV TID for 5 days
Composition-
METRONIDAZOLE.
. Metronidazole
belongs to Nitro imidazole group of antibiotics, is used to treat
gastrointestinal infections, skin and blood infections.
Mechanism of action:
Metronidazole diffuses into the organism, inhibits protein synthesis by
interacting with DNA and causing a loss of helical DNA structure and strand
breakage. Therefore, it causes cell death in susceptible organisms.
Based on the
above study metronidazole when combined with another antimicrobial agent is
more effective in the treatment of complicated intra-abdominal infections (particularly
those caused by ENTEROBACTERIACEAE MEMBERS as they are resistant to
carbipenem).
3) ING.
AMIKACIN 500 mg IV BD for 5days
. AMIKACIN is
an amino glycoside antibiotic used in the treatment of serious bacterial
infections.
Mechanism of
action: The primary mechanism of action of amikacin is the
same as that for all aminoglycosides. It binds to bacterial 30S ribosomal
subunits and interferes with mRNA binding and tRNA acceptor sites, interfering
with bacterial growth.
All the above
three antibiotics are given to control infection and prevent sepsis in the
patient.
4) ING.
OCTREOTIDE 100 mg SC, BD
Octreotide is a
long acting analogue of Somatostatin
. It inhibits
exocrine secretion of the pancreas, also has anti-inflammatory and
cytoprotective effects.
Mechanism of
action: octreotide decreases the release of growth stimulating hormones,
decreases blood flow to the digestive organs, and inhibits the release of
digestive hormones such as serotonin, gastrin, vasoactive intestinal peptide,
secretin, motilin, and pancreatic polypeptide
EFFICACY -
Octeotride based on several studies did not provide any symptomatic relief or
better cure when compared to other drugs. However, it played a significant role
in reducing SERUM AMYLASE AND LIPASE LEVELS.
5) ING. PANTOP
40 mg IV, OD
. Pantoprazole
a proton pump inhibitor, is known to have pancreatic anti secretory effect.
. Oxidative
stress is common in acute pancreatitis- Pantoprazole has an inhibitory
effect on hydroxyl radicals (free radicals)- thereby reduces the progression of
the disease and helps in reducing oxidative stress.
. PPZ
treatment also reduces tissue infiltration of inflammatory cells and acinar
cell necrosis in severe AP.
6) ING.
TRAMADOL in 100 ml NS IV, OD
Tramadol is an
opioid analgesic used to relieve severe pain in acute pancreatitis.
Mechanism of
action: Tramadol is a centrally acting analgesic with a multimode of action.
It acts on serotonergic and noradrenergic nociception, while its metabolite
O-desmethyltramadol acts on the µ-opioid receptor. Its analgesic potency is
claimed to be about one tenth that of morphine.
7)ING. THIAMINE
100 mg in 100 ml NS IV, TID*
. Thiamine -
Vitamin B1 supplement.
. As the
patient is on TPN there is a chance of B1 deficiency
. Wernicke’s
encephalopathy (due to B1 deficiency) has been noted in several cases of pancreatitis so
to prevent this Thiamine is given as a prophylactic measure
8) TPN (Total
Parenteral Nutrition)
(TPN) is
a method of feeding that bypasses the gastrointestinal tract. Fluids are given
intravenously to provide nutrients the body needs. The method is used when
a person cannot or should not receive feedings or fluids by mouth.
Parenteral
nutrition is used to prevent malnutrition in patients who are unable to obtain
adequate nutrients by oral or enteral
routes.
9) IV NS
/ RL at the rate 12l ml per hour
MY APPROACH TO
THIS PATIENT AS A TREATING PHYSICIAN:
-When the
patients present with the complaints of pain abdomen and vomiting, along with
fever, burning micturition, certain investigations must be done.
- First, a
general examination must be done, including inspection, percussion, palpation
and auscultation of the abdomen.
-Other
investigations are CBP (Complete Blood Picture), LFT (Liver Function tests), RFT
(Renal Function Test), Urine analysis, Serum amylase, ABG (Arterial Blood Gas),
Pleural tapping.
-Some imaging
studies like, contrast enhanced CT and chest x-ray should be taken as well.
-Now depending
on the diagnosis based on the results, chemotherapy must be started. In the
case of pancreatitis in this patient, the following treatment can be given.
-- Antibiotic
like MEROPENAM, METROGYL, AMIKACIN
-- Fluid levels
should be maintained with RL or NS
--Somatostatin
analogue like SOMATOSTATIN, decreases the exocrine secretion in the pancreas
-- Proton pump
inhibitor
--Vitamins such
as Thiamine
--Anti-analgesic
such as TRAMADOL
CASE: https://nehae-logs.blogspot.com/2021/05/case-discussion-on-25-year-old-male.html
QUESTION: What is causing the patient's dyspnoea? How is
it related to pancreatitis?
Pancreatitis
is associated with shortness of breath( https://www.mayoclinic.org/diseases-conditions/pancreatitis/symptoms-causes/syc-20360227#:~:text=Breathing%20problems.,fall%20to%20dangerously%20low%20levels )
Acute
pancreatitis is associated with release of inflammatory factors which the lungs,
fluid accumulation which is also associated with pancreatitis (the patient was
diagnosed pleural effusion) results in shortness of breath.
QUESTION: Name possible reasons why the patient has developed a
state of hyperglycaemia.
1.
Pancreatitis
damages cells that produce insulin and glucagon which are hormones that control
the levels of blood sugar. Insufficiency of these hormones can lead to
hyperglycaemia
2.
Patient
is a known alcoholic with increased consumption since 2 months (2 litres of
toddy everyday) which could also be a cause of diabetes in the patient. But the
patient was never tested before he came to our OPD and did not recall any
notable signs.
QUESTION: What is the reason for his elevated
LFTs? Is there a specific marker for Alcoholic Fatty Liver disease?
Excess
alcohol consumption is known to elevate LFT’s. alcohol is a known hepatotoxin
which effects liver functioning and there is no certain linear relation between
the amount consumed and the stage of liver damage.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4155359/
Sensitivity and
specificity of biomarkers in detecting harmful or heavy alcohol consumption
|
Biomarker |
AST |
ALT |
MCV |
CDT |
CDT + GGT |
CDT + GGT + MCV |
|
Sensitivity |
47%-68% |
32%-50% |
45%-48% |
63%-84% |
83%-90% |
88% |
|
Specificity |
80%-95% |
87%-92% |
52%-94% |
92%-98% |
95%-98% |
95% |
AST: Aspartate aminotransferase; ALT: Alanine aminotransferase;
MCV: Mean corpuscular volume; CDT: Carbohydrate-deficient transferring; GGT:
Gamma-glutamyltranspeptidase. (source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4155359/ )
GGT and CDT are usually taken as specific markers for ALD
QUESTION: What is the line of treatment in this patient?
plan of action
and Treatment:
Investigations:
✓
24 hour urinary protein
✓
Fasting and Post prandial Blood glucose
✓
HbA1c
✓
USG guided pleural tapping
Treatment:
• IVF: 125
mL/hr
• Inj PAN 40mg
i.v OD
• Inj ZOFER 4mg
i.v sos
• Inj Tramadol
1 amp in 100 mL NS, i.v sos
• Tab Dolo
650mg sos
• GRBS charting
6th hourly
• BP charting
8th hourly
CASE: https://chennabhavana.blogspot.com/2021/05/general-medicine-case-discussion-1.html
QUESTION: What is the most probable diagnosis in
this patient?
-Differential
Diagnosis:
a)
Ruptured
Liver Abscess.
b)
Organized
Intraperitoneal Hematoma.
c)
Organized
collection secondary to Hollow Viscous Perforation.
d)
Free
fluid with internal echoes in Bilateral in the Sub diaphragmatic space.
e)
Grade
3 RPD of right Kidney
-The
most probably diagnosis is there is abdominal hemorrhage. This will give
reasoning to the abdominal distention, and the blood which is aspirated.
QUESTION: What was the cause of her death?
-After
getting discharged from the hospital, the patient went to Hyderabad and
underwent an emergency laparotomy surgery. The patient passed away the next
day. Cause of her death can be due to complications of laparotomy surgery such
as, hemorrhage (bleeding), infection, or damage to internal organs.
QUESTION: Does her NSAID abuse have something to do
with her condition? How?
-NSAID-induced
renal dysfunction has a wide spectrum of negative effects, including decreased
glomerular perfusion, decreased glomerular filtration rate, and acute renal
failure. Chronic NSAIDs use has also been related to hepatotoxicity. While the
major adverse effects of NSAIDs such as gastrointestinal mucosa injury are well
known, NSAIDs have also been associated with hepatic side effects ranging from
asymptomatic elevations in serum aminotransferase levels and hepatitis with
jaundice to fulminant liver failure and death.
SYSTEM: NEPHROLOGY
CASE: https://kavyasamudrala.blogspot.com/2021/05/medicine-case-discussion-this-is-online.html
QUESTION: What could be the reason for his SOB?
This
patient underwent a TURP around two months ago, post which he came back to the
hospital with Hyponatremia, and elevated creatinine levels (5.2 mg/dl). These
were both corrected and he was discharged.
After
discharge, he came for routine testing about 1 week later, with elevated
creatinine levels (6.2 mg/dl), and then presented to the hospital with SOB on
exertion with a serum creatinine level raised to 10 mg/dl.
The
increased creatinine levels are known to cause shortness of breath.
QUESTION: Why does he have intermittent
episodes of drowsiness?
In
this case, post TURP in the patient he presented to the hospital with
drowsiness and excessive sleep that attenders felt difficult to wake him
up from sleep and attenders were regularly monitoring his BP, which was found
to be fluctuating and patient was brought to the hospital. The patient was diagnosed with hyponatremia.
The common symptoms of hyponatremia related to this case are- headache,
confusion, loss of energy, drowsiness and fatigue. This could have been the
cause for drowsiness.
QUESTION:
Why did he complaint of fleshy
mass like passage in his urine?
The patient in this case has
a history of dysuria and urine is cloudy in appearance. On investigation, there
is a presence of pus cells in the urine. The patient has an indication of
hydronephrosis, which is a condition that typically occurs when the kidney swells
due to urine failing to properly drain from the kidney to the bladder. Due to
stasis of fluid, these patients become predisposed to development of urinary
tract infection (UTI), which can be the cause of fleshy type masses or gritty
particles in the urine.
QUESTION:
What are the complications of TURP that he may have had?
ANS. Some possible complications
may include:
a) Bladder injury
b) Bleeding
c) Blood in the urine after
surgery
d) Electrolyte abnormalities
e) Infection
f) Painful or difficult
urination
g) Retrograde ejaculation (when
ejaculate goes into the bladder and not out the penis)
QUESTION: What could be the reason for
his SOB?
This
patient underwent a TURP around two months ago, post which he came back to the
hospital with Hyponatremia, and elevated creatinine levels (5.2 mg/dl). These
were both corrected and he was discharged.
After
discharge, he came for routine testing about 1 week later, with elevated
creatinine levels (6.2 mg/dl), and then presented to the hospital with SOB on
exertion with a serum creatinine level raised to 10 mg/dl.
The
increased creatinine levels are known to cause shortness of breath.
QUESTION: Why does he have intermittent
episodes of drowsiness?
In
this case, post TURP in the patient he presented to the hospital with
drowsiness and excessive sleep that attenders felt difficult to wake him
up from sleep and attenders were regularly monitoring his BP, which was found
to be fluctuating and patient was brought to the hospital. The patient was diagnosed with hyponatremia.
The common symptoms of hyponatremia related to this case are- headache,
confusion, loss of energy, drowsiness and fatigue. This could have been the
cause for drowsiness.
QUESTION:
Why did he complaint of fleshy
mass like passage in his urine?
The patient in this case has
a history of dysuria and urine is cloudy in appearance. On investigation, there
is a presence of pus cells in the urine. The patient has an indication of
hydronephrosis, which is a condition that typically occurs when the kidney swells
due to urine failing to properly drain from the kidney to the bladder. Due to
stasis of fluid, these patients become predisposed to development of urinary
tract infection (UTI), which can be the cause of fleshy type masses or gritty
particles in the urine.
QUESTION:
What are the complications of TURP that he may have had?
ANS. Some possible complications
may include:
a) Bladder injury
b) Bleeding
c) Blood in the urine after
surgery
d) Electrolyte abnormalities
e) Infection
f) Painful or difficult
urination
g) Retrograde ejaculation (when
ejaculate goes into the bladder and not out the penis)
QUESTION: What could be the reason for his SOB?
This
patient underwent a TURP around two months ago, post which he came back to the
hospital with Hyponatremia, and elevated creatinine levels (5.2 mg/dl). These
were both corrected and he was discharged.
After
discharge, he came for routine testing about 1 week later, with elevated
creatinine levels (6.2 mg/dl), and then presented to the hospital with SOB on
exertion with a serum creatinine level raised to 10 mg/dl.
The
increased creatinine levels are known to cause shortness of breath.
QUESTION: Why does he have intermittent
episodes of drowsiness?
In
this case, post TURP in the patient he presented to the hospital with
drowsiness and excessive sleep that attenders felt difficult to wake him
up from sleep and attenders were regularly monitoring his BP, which was found
to be fluctuating and patient was brought to the hospital. The patient was diagnosed with hyponatremia.
The common symptoms of hyponatremia related to this case are- headache,
confusion, loss of energy, drowsiness and fatigue. This could have been the
cause for drowsiness.
QUESTION:
Why did he complaint of fleshy
mass like passage in his urine?
The patient in this case has
a history of dysuria and urine is cloudy in appearance. On investigation, there
is a presence of pus cells in the urine. The patient has an indication of
hydronephrosis, which is a condition that typically occurs when the kidney swells
due to urine failing to properly drain from the kidney to the bladder. Due to
stasis of fluid, these patients become predisposed to development of urinary
tract infection (UTI), which can be the cause of fleshy type masses or gritty
particles in the urine.
QUESTION:
What are the complications of TURP that he may have had?
ANS. Some possible complications
may include:
a) Bladder injury
b) Bleeding
c) Blood in the urine after
surgery
d) Electrolyte abnormalities
e) Infection
f) Painful or difficult
urination
g) Retrograde ejaculation (when
ejaculate goes into the bladder and not out the penis)
CASE: https://drsaranyaroshni.blogspot.com/2021/05/an-eight-year-old-with-frequent.htm
QUESTION:
Why is the child excessively hyperactive without much of social
etiquettes?
ANS. According to the case
history, the patient, in this case an 8-year-old boy, is excessively
hyperactive, impulsive, does not have proper social etiquettes as is expected
of his age, too active to pay any attention at school, talk so fast that even
comprehending sentences becomes quite difficult. These issues are ongoing in
the boy, and are prominent enough to be negatively affecting his daily life. This
indicates towards the boy possibly having ADHD (attention deficit hyperactivity
disorder), a mental health disorder that can cause above-normal levels of
hyperactive and impulsive behaviors. People with ADHD may also have
trouble focusing their attention on a single task or sitting still for long
periods of time.
People who have ADHD present with the
combination of these symptoms:
a)
Overlook
or miss details, make careless mistakes in schoolwork, at work, or during other
activities
b)
Have
problems sustaining attention in tasks or play, including conversations,
lectures, or lengthy reading
c)
Seem
to not listen when spoken to directly
d)
Fail
to not follow through on instructions, fail to finish schoolwork, chores, or
duties in the workplace, or start tasks but quickly lose focus and get easily
sidetracked
e)
Avoid
or dislike tasks that require sustained mental effort, such as schoolwork or
homework.
f)
Lose
things necessary for tasks or activities, such as school supplies, pencils,
books, tools, wallets, keys, paperwork, eyeglasses, and cell phones
g) (Reference link- https://www.nimh.nih.gov/health/publications/attention-deficit-hyperactivity-disorder-adhd-the-basics/)
Before ADHD is made as a proper
diagnosis, these activities can often be interpreted as the child being
hyperactive, out of control, and lacking in social etiquette.
QUESTION:
Why doesn't the child have the excessive urge of urination at night time?
ANS. The child in this case has
gotten a series of tests done in order to come to a conclusion about his
diagnosis.
a)
They
have done a complete urine exam, a urine culture and sensitivity test, and
checked levels of serum electrolyte and they were normal.
b)
From
the history of excessive hyperactivity, impulsiveness, lacking of attentivity,
a thought goes towards Attention Deficit Hyperactivity Disorder (ADHD) and in
turn towards the association urination disorders. Studies indicate that
children with ADHD have a higher tendency to lack bladder control, and are
prompted to go to the bathroom more frequently.
c)
Since
the child does not get the urgency to urinate when he is asleep, there can be a
chance of the manifestation being psychosomatic, or as a result of an
undiagnosed anxiety disorder, or a stressor triggering this manifestation.
When
you feel anxious, your body’s fear response can be triggered, overwhelming your
bladder’s mechanisms for retaining urine, causing you to want to urinate. The
child may be free from the triggers while asleep, especially because he does
not have a history of nocturnal enuresis, thus enabling him to sleep well
through the night.
QUESTION:
How would you want to manage the patient to relieve him of his symptoms?
ANS. The diagnosis of the child is
leaning towards the possibility of a psychosomatic overactive bladder, which
can be triggered by various stressors or the possibility of the child having
undiagnosed ADHD, a conclusion based on history of his behavior. In either of
these cases, change in the daily habits and behavior, along with conservative
therapy such as bladder exercises can go a long way before doing medical or
surgical intervention.
-The most common treatment options
include bladder retraining and pelvic floor exercises.
-
Bladder
retraining involves putting the child on a “voiding schedule” where they go to
the restroom to urinate on a schedule. This helps to slowly train the bladder
to hold more and more urine, as it is designed to.
-
Pelvic
floor exercises provide a way to strengthen the muscles that are used to slow
and stop the flow of urine and prevent wetting.
If the above methods do not work drugs like oxybutynin can help in controlling an overactive bladder.
-
INFECTIOUS DISEASES:
CASE: https://vyshnavikonakalla.blogspot.com/2021/05/a-40-year-old-lady-with-dysphagia-fever.html
QUESTION: Which clinical history and physical
findings are characteristic of tracheoesophageal fistula?
-In
adults, the characteristic history is recurrent pneumonia, hemoptysis, and
coughing after eating.
- In
children, the features found in cases of congenital tracheoesophageal fistula
are- there is frothy, white bubbles in the mouth, coughing or choking when feeding,
vomiting, blue color of the skin (cyanosis), especially when the baby is
feeding, difficulty breathing.
- The
physical findings are, in the presence of TEF, abdominal distention may occur
secondary to collection of air in the stomach.
QUESTION: What are the chances of this patient
developing immune reconstitution inflammatory syndrome? Can we prevent
it?
- Immune
reconstitution inflammatory syndrome (IRIS) is a condition seen in some
cases of AIDS or immunosuppression, in which the immune system begins
to recover, but then responds to a previously acquired opportunistic infection with
an overwhelming inflammatory response that paradoxically makes the
symptoms of infection worse.
-There
are chances that this patient can develop IRIS due to the patient being RVD
positive. She is more susceptible to any infection and therefor prone to
reinfection. To prevent IRIS, the most effective method is to involve the
initiation of ART before immunosuppression is advanced. IRIS is uncommon in
individuals who initiate antiretroviral treatment with a CD4+ T-cell count
greater than 100 cells/uL. Aggressive efforts should be made to detect
asymptomatic mycobacterial or cryptococcal disease prior to the initiation of
ART, especially in areas endemic for these pathogens and with CD4 T-cell counts
less than 100 cells/uL.
INFECTIOUS DISEASE AND HEPATOLOGY
CASE: https://kavyasamudrala.blogspot.com/2021/05/liver-abscess.html
QUESTION: Do you think drinking locally made alcohol caused liver abscess in this patient due to predisposing factors present in it? What could be the cause in this patient?
Patient
is toddy drinker since 30 years and by occupation he is a palm tree climber. Toddy
is locally fermented beverage and can be contaminated with various organisms. The
organism that is known to cause liver abscess is enatamoeba histolytica. The patient
belongs to the low socio-economic group and is malnourished which favours the survival
of the parasite
QUESTION: What is the etiopathogenesis of
liver abscess in a chronic alcoholic patient? (since 30 years - 1 bottle per
day)
Alcohol
causes AMOEBIC LIVER ABSCESS(ALA) through a multitude of mechanisms:
a)
Alcohol
induced hepatic dysfunction
b)
It
lowers body resistance and suppresses immune mechanisms in the habitual
consumers.
c)
Locally
prepared alcohol (toddy) when brewed in unhygienic conditions may be
contaminated by pathogens (bacteria, parasites- ENTAMOEBA HISTOLYTICA.)
d)
Toddy
has very less alcoholic content (< 5%) - this favours the survival of
Entamoeba and promotes the conversion of latent forms to virulent forms
resulting in more symptomatic cases.
alcohol-induced
hepatic dysfunction and possible suppression of amoebistatic immune mechanisms
by substances in the beverages could also be attributed in the mechanism
QUESTION:
Is liver abscess more common in
right lobe?
Liver
abscess is more common in right lobe than left lobe. The ratio is 2:1.
Liver abscess is more
common in the right lobe than left lobe because
a)
The
right hepatic lobe receives blood from both the superior mesenteric and portal
veins, whereas the left hepatic lobe receives inferior mesenteric and splenic
drainage
b)
It
also contains a denser network of biliary canaliculi and overall more hepatic
mass.
QUESTION:
What are the indications for
ultrasound guided aspiration of liver abscess?
Indications for
aspiration of a liver abscess include the following:
a)
Presence
of a left lobe abscess of more than 10cm in diameter.
b)
Pain
and impending rupture.
c)
Abscess
that does not respond to medical treatment within 3-5 days.
CASE: https://63konakanchihyndavi.blogspot.com/2021/05/case-discussion-on-liver-abcess.html
QUESTION: Cause of liver abscess in this patient?
Patient
is an occasional Toddy drinker.
Toddy when collected in unhygienic environment, might get contaminated with
pathogens such as bacteria, parasites (Entamoeba histolytica).
These
pathogens though portal circulation reach the liver and might result in ABSCESS
formation in the patient.
QUESTION:
How do you approach this patient?
.
When patient presents with chief complaints of abdominal pain, fever -
1.
Detailed
history regarding each of the symptom should be taken.
2.
General
examination to know the overall health status should be carried out.
3.
Following
general examination, systemic examination (CVS, RESPIRATORY, PER ABDOMEN, CNS)
should be done.
Patient’s
symptoms point out to the involvement of GASTROINTESTINAL SYSTEM, therefore
special emphasis should be on per abdominal examination.
4. Through history and examination,
we arrive at provisional diagnosis.
5. To confirm the
diagnosis, investigations, imaging tests should be taken.
6. For this patient
based on his symptomatology, the following investigations should be done.
CBP,
LIVER FUNCTION TESTS, RENAL FUNCTION TESTS, URINE ANALYSIS.
7. Imaging tests- CXR,
USG abdomen.
Based on the results of
these the diagnosis can be confirmed; treatment can be initiated.
This
patient is diagnosed with LIVER ABSCESS (by the above approach), the following
treatment can be given.
.
In practice an empirical treatment is given to treat both amoebic and pyogenic
liver abscess -
This includes use of
Broad spectrum antibiotics (for pyogenic liver abscess), Metronidazole (for
amoebic liver abscess)
.
Analgesics and anti inflammatory drugs -to relieve pain and fever.
.
Multivitamin supplements
.
Saline infusion- to maintain fluid levels.
All
the above medicines should be given for 7- 10
days.
Following
this review, the patient and see if there is any improvement.
USG
abdomen should be done se if the abscess is resolving.
Investigations
(CBP, LFT, RFT) should be done to check for the improvement.
If
the abscess did not resolve ULTRASOUND GUIDED ASPIRATION SHOULD BE DONE.
QUESTION:
Why do we treat here; both
amoebic and pyogenic liver Abscess?
The presentation for
both amoebic, pyogenic liver abscess is the same I.e, pain abdomen, fever,
constitutional symptoms like nausea and vomiting, loss of appetite, in some
cases there may be pulmonary symptoms.
INVESTIGATIONS-
There
is leucocytosis, elevated alkaline phosphatase, ALT, AST
USG-a
hypo echoic mass for both type of abscess.
Amoebic
and pyogenic liver abscess can be differentiated only by culture and sensitivity
of the aspirate obtained by USG GUIDED ASPIRATION OF THE ABSCESS.
USG
GUIDED ASPIRATION has the following risk factors associated with it:
1) if
abscess is thin walled there is a risk of rupture.
2)if
abscess is on the posterior aspect of the liver, it will not be accessible.
3)there
is also a risk of bleeding.
.
Blood culture taken prior to the administration of antibiotics is helpful for
identifying the causative organism but as this
patient had already taken antimicrobials before he came to the hospital, there
is severe abdominal pain treatment is started immediately without a blood
culture report.
Considering
that it is difficult to distinguish amoebic liver abscess from pyogenic liver
abscess,
We
treat both forms of Liver abscess empirically using-
·
Broad
spectrum antibiotics- a combination of penicillin, cephalosporin,
ahminoglycosides
·
Metronidazole-
has both antibacterial and antiprotozoal activity.
Liver
abscess: diagnostic and management issues found in ...https://academic.oup.com
› bmb › article
This
article highlights the difficulties in distinguish the two forms of liver
abscess.
QUESTION: Is there a way to confirm the
definitive diagnosis in this patient?
Liver
abscess can be confirmed by USG ABDOMEN - it presents as single / multiple,
round / oval, hypoechoic - hyper echoic mass more commonly is
the right lobe of the liver.
However,
USG cannot differentiate an amoebic liver abscess from pyogenic liver abscess.
For
this
·
Blood
culture
·
USG
guided aspiration of the abscess should be done.
This
aspirate should be subjected to antigen testing for –
Subjected to
microbiological culture and sensitivity - to identify pyogenic organisms.
INFECTIOUS DISEASE (MUCORMYCOSIS)
CASE: https://manikaraovinay.blogspot.com/2021/05/50male-came-in-altered-sensorium.html
QUESTION: What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary aetiology of the patient's problem?
1. 3
years ago- diagnosed with hypertension
2. 21
days ago- received vaccination at local PHC which was followed by fever
associated with chills and rigors, high grade fever, no diurnal variation which
was relieved on medication
3. 18
days ago- complained of similar events and went to the the local hospital, it
was not subsided upon taking medication(antipyretics)
4. 11
days ago - c/o
Generalized weakness and facial puffiness and periorbital oedema. Patient was
in a drowsy state
5. 4 days
ago-
a. patient
presented to casualty in altered state with facial puffiness and periorbital oedema
and weakness of right upper limb and lower limb
b. towards
the evening patient periorbital oedema progressed
c. serous
discharge from the left eye that was blood tinged
d. was
diagnosed with diabetes mellitus
6. patient
was referred to a government general hospital
7. patient
died 2 days ago
patient
was diagnosed with diabetic ketoacidosis and was unaware that he was diabetic
until then. This resulted in poorly controlled blood sugar levels. The patient
was diagnosed with acute oro rhino orbital mucormycosis . rhino cerebral
mucormycosis is the most common form of this fungus that occurs in people with
uncontrolled diabetes ( https://www.cdc.gov/fungal/diseases/mucormycosis/definition.html ) the
fungus enters the sinuses from the environment and then the brain.
The
patient was also diagnosed with acute infarct in the left frontal and temporal
lobe. Mucormycosis is associated with the occurrence of CVA ( https://journal.chestnet.org/article/S0012-3692(19)33482-8/fulltext#:~:text=There%20are%20few%20incidences%20reported,to%20better%20morbidity%2Fmortality%20outcomes. )
QUESTION: What is the efficacy of drugs used along
with other non-pharmacological treatment modalities and how would you approach
this patient as a treating physician?
The proposed management of the patient was –
1. inj.
Liposomal amphotericin B according to creatinine clearance
2. 200mg Iitraconazole
was given as it was the only available drug which was adjusted to his
creatinine clearance
3. Deoxycholate
was the required drug which was unavailable
https://pubmed.ncbi.nlm.nih.gov/23729001/ this
article talks about the efficacy and toxicity of different formulations of
amphotericin B
along
with the above mentioned treatment for the patient managing others symptoms is
also done by-
I.
Management of diabetic ketoacidosis –
(a) Fluid
replacement- The fluids will
replace those lost through excessive urination, as well as help dilute the
excess sugar in blood.
(b) Electrolyte
replacement-The absence of insulin
can lower the level of several electrolytes in blood. Patient will receive
electrolytes through a vein to help keep the heart, muscles and nerve cells
functioning normally.
(c) Insulin
therapy- Insulin reverses
the processes that cause diabetic ketoacidosis. In addition to fluids and
electrolytes, patient will receive insulin therapy
QUESTION:
What are the postulated reasons for a
sudden apparent rise in the incidence of mucormycosis in India at this point of
time?
Mucormycosis is may be being triggered by the
use of steroids, a life-saving treatment for severe and critically ill Covid-19
patients. Steroids reduce inflammation in the lungs for Covid-19 and appear to
help stop some of the damage that can happen when the body's immune system goes
into overdrive to fight off coronavirus. But they also reduce immunity and push
up blood sugar levels in both diabetics and non-diabetic Covid-19 patients.
With the COVID-19 cases rising
in India the rate of occurrence of mucormycosis in these patients is increasing
QUESTION 9
http://medicinedepartment.blogspot.com/2021/05/covid-case-report-logs-from-may-2021.html?m=1
1) Sort out these detailed patient case report logs into a single web page as a master chart
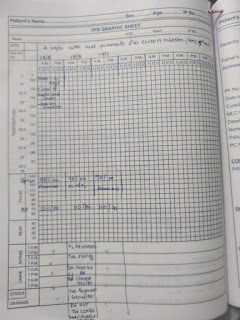
Comments
Post a Comment