63 YEAR OLD MALE WITH HYPOGLYCEMIA
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your
valuable comments on comment box is welcome
22-02-2022
CASE:
A 63 year old male came to the hospital with the complaints of discomfort, excessive sweating, dizziness
HISTORY OF PRESENTING ILLNESS:
The patient was apparently asymptomatic one day ago when he developed discomfort and excessive sweating early in the morning he then lost consciousness. He was then brought to the hospital by the attender. He was brought in an ambulance and on the way to the hospital he was given glucose as his sugars were low. He gained consciousness after administering glucose.
He had no h/o of fever, cough, cold, seizures etc.
PAST HISTORY:
The patient is a known diabetic since 18 years.
In 2019, the patient experienced a skin prick on his great toe of left leg in the farm, which eventually developed into an ulcer. After the prick the patient didn’t address the wound for a week after which he went to a local doctor who advised him a TT injection. The wound was left open as he was diabetic. The wound started gradually growing in size and involved the medial aspect of the foot and the first few toes.

After the ulcer involved most of his leg he was taken to a hospital where he underwent an amputation of his first two toes. After the amputation the infection persisted and he underwent further investigations. A doppler was done.



He had fever and cough during this period. He underwent a percutaneous coronary intervention on his left lower limb following which the foot was debrided and vacuum assisted closure was done.
Four days after the discharge after the amputation the patient experienced a similar episode to yesterday. He experienced discomfort, excessive sweating and his skin felt cold.
He was ventilated and was in the hospital for 15 days.
He was discharged and the wound dressing was continued at home.
In 2020, the patient had another episode of similar complaints and had seizures , he was given sugar water after he regained consciousness and he was not taken to the hospital.
In 2021, September the patient had complaints of anasarca for 4 days which was sudden in onset and progressive, decreased urine output which ceased completely in 4 days, he did not pass faeces for 4 days, he had abdominal distention for 4 days and it was also progressive. He also had shortness of breath (grade 3), he had vomiting after meals. The patient was taken to the hospital where he underwent dialysis and this was followed by 20 sessions of dialysis in 2 months ( twice a week).
The patient is now receiving dialysis twice a week .
FAMILY HISTORY:
There are no similar complaints in the family. His mother was diagnosed with cancer when he was young.
PERSONAL HISTORY:
Diet : mixed diet
Appetite : has three meals a day and his appetite increases and decreases occasionally
Sleep: initially he slept 4-5 hours a day and after dialysis he sleeps 2-3 hrs a day
Bowel: regular
Addictions: consumed alcohol occasionally and stoped 3 years ago
Allergies: none
He was previously a farmer and has stopped working since the amputation
He stays at home and goes out occasionally
GENERAL EXAMINATION :
The patient was conscious, coherent and co - operative.
He is well oriented to time, place and person.
Pallor was present
No icterus
No clubbing
No cyanosis
No generalized lymphadenopathy
Skin is dry and rough
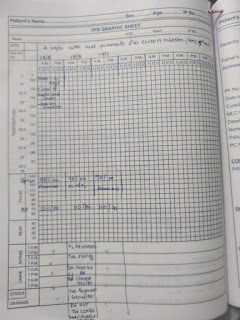
GRBS ON DAY 1: 138 (Morning 11 am)



VITALS:
Temp - afebrile
BP - 140/90 mmhg
PR - 92 bpm
RR - 18 cpm
SpO2 - 99% at RA
SYSTEMIC EXAMINATION:
CVS: S1 and S2 are heard
No thrills and murmurs
RESPIRATORY SYSTEM:
INSPECTION:
Chest wall is bilaterally symmetrical and elliptical in shape
No chest wall and spine abnormalities
No dilated veins, sinuses
Scars present on the base on the right neck
PERCUSSION:
Areas: all areas are bilaterally resonant
Supra clavicular
Infra clavicular
Mammary
Axillary
Infraxillary
Supra-scapular
Scapular
Infra-scapular
PALPATION:
No local rise of temperature, no tenderness
Trachea is centrally placed
No tactile fremitus
No vocal fremitus
AUSCULTATION:
Normal vesicular breath sounds are heard
BAE present
No dyspnea
ABDOMEN:
INSPECTION:
Shape of abdomen: scaphoid
Scar present above the umbilicus
PERCUSSION:
no fluid thrill or dullness
PALPATION:
No tenderness, no palpable mass, no free fluid, liver and spleen are not palpable
AUSCULTATION:
Normal bowel sounds heard
CENTRAL NERVOUS SYSTEM:
Speech: normal
No neck stiffness
Cranial nerves -N
Gait: walks with a walking stand since the amputation
Sensory system- normal
Motor system: tone: normal
Power: normal
Reflexes: normal



Comments
Post a Comment